

Read time: ~20 minutes.
Table of Contents
- Introduction
- Definition and Health Benefits of Resistance Training
- Background of Injuries in Resistance Training
- Injury Sites and Severity
- Risk factors
- A Side Note about Injury & Pain
- Exercise Technique and Injury Risk
- Managing “Risk”
Introduction
You've probably heard this before "Keep your back straight, or you'll injure yourself!", especially if you've worked with a personal trainer or physiotherapist before. While this statement holds true to a certain extent, it is imperative that we delve into the underlying research to determine its validity. Failing to stay current with the latest research would be both ignorant and a disservice to the people we work with. Therefore, it is crucial to avoid making sweeping statements without first reviewing the available evidence.
By the end of this read, you should have acquired new, actionable knowledge that can be applied in your training. Furthermore, this would help you to seek more information when someone makes a similar statement. For this article, the terms Resistance Training & Strength training is used synonymously and mean the same thing. I suggest reading this article in parts and not all in one go, as it can get quite overwhelming. With that in mind, let's dive right into today's article.
Definition and Health Benefits of Resistance Training
Resistance training or strength training (a term which I don’t really like) is an exercise type that has gained popularity among adults in recent decades (partly contributed by social media), mostly for its role in improving athletic performance by increasing muscular strength, power, speed, hypertrophy (muscle growth), local muscular endurance, motor performance, balance, and coordination 1. There is a lot of research supporting the use of resistance training as they provide a vast amount of health benefits 2 that will benefit you into old age, such as the preservation of functional mobility, muscle strength, muscle mass, bone mass, and reduced risk of falls 3–6. This is provided the trainee continues to participate in resistance training throughout his/her lifespan as much as possible and at an intensity within his/her abilities.
As a matter of fact, resistance training is now widely advocated by local state health organizations such as the Ministry of Health (MOH), Health Promotion Board (HPB) in Singapore, and organizations abroad such as the American College of Sports Medicine (ACSM), and the American Heart Association (AHA). They recommend that most individuals, even those with cancer 7, diabetes 8–10, cardiovascular11, and neuromuscular disease 12,13, participate in muscle-strengthening activities that work all major muscle groups for 2 or more days a week.
Background of Injuries in Resistance Training
Given the fact that Resistance training involves high-intensity loaded activities, shear, and compressive forces exerted on joints and other connective tissue can be large. When we look at epidemiological research (where researchers study the distribution and determinants of health-related states or events in specified populations) of injuries across weight-training sports. These sports include weightlifting, powerlifting, bodybuilding, strongman, CrossFit, and the highland games (see Fig. 1 ) A systematic review14 showed that weight-training sports have a relatively lower rate of injury compared to common team sports such as soccer, basketball, etc.
Among the weight-training sports, bodybuilding had the lowest injury rates (0.24-1 injury per 1000h of training), whereas strongman and highland games had the highest rates of injury (4.5-6.1 and 7.5 injuries per 1000h of training respectively)14,15. To put things into perspective, that’s 0.12-0.7 injuries per lifter, per year, for bodybuilding! When we compare it to professional team sports like soccer which has a total injury incidence rate of 2.48 to 9.8 injuries per 1000h of exposure16, the difference is astounding. Therefore, resistance training in general, especially when done recreationally, is safe for most people, as being involved in competitive weight-training sports often adds another layer of complexity to predicting injury risk. In fact, a meta-analysis examining 6 studies showed that supported resistance training as a training modality to prevent injuries in athletes participating in team sports, and that a higher resistance training volume and intensity were closely related to a reduction in sports injury risk17.
Based on the above, we can safely conclude that the health benefits of lifting weights outweigh the extremely low odds of sustaining an injury in the weight room (provided you approach lifting in a sensible, reasonable manner and not attempt crazy, outrageous ways of lifting like what you see on social media, see Fig 2).

Source: Keogh & Winwood (2017)

Source: YouTube
Injury Sites and Severity
When we look at the research, common injury sites in these sports include the shoulder, knee, and lower back while the type of injuries include muscle strains, tendinopathy (also known as tendon overuse injuries), and ligament sprains. Additionally, most of these injuries stated in the studies were of mild to moderate severity.
Risk factors
We can categorize risk factors into extrinsic and intrinsic, both of which predispose an athlete or individual to injury in weight-training sports. Going further, these risk factors can be separated into modifiable and non-modifiable, where the former is addressed, as the name itself suggests, through specific warm-ups, or injury prevention protocols whereas relevant non-modifiable factors can be described to individuals who are keen on participating in these sports. However, little has been studied about the risk factors of injuries in weight training, particularly extrinsic risk factors (i.e. training environment, rules of the sport, and coaching method) 14,18. Furthermore, it was also suggested by Keogh & Winwood (2017) that intrinsic risk factors such as age, gender, competitive standard, and body weight class only affect the injury epidemiology of these sports only to a minor extent. Thus, the notion that using proper technique or ‘form’ would result in a reduced risk of injury is an oversimplification, as many factors go into identifying individuals at risk of injury.
Nonetheless, knowing what constitutes proper technique also requires a basic understanding of human anatomy such as which muscle groups are involved in a specific movement and limb kinematics (forces going through joints and muscles. As this is not within the scope of today’s topic, it will be discussed in detail over multiple articles in the future, so stay posted! Now, with a brief understanding of injuries in weight-training sports, let’s move on to the meat of today’s topic.
A Side Note about Injury & Pain
I’d like to go off tangent for a little bit and briefly discuss injuries and pain because it will help you understand the content that lies after this. Let’s face it, nobody wants to get injured - expensive medical bills, the hassle of going to medical appointments, difficulty performing simple day-to-day tasks due to pain, and not being able to do activities you were previously able to. If we want to prevent injury, we need to broaden our understanding of what an injury is. According to the International Olympic Committee Injury and Illness Epidemiology Consensus group19, it is defined as “tissue damage or other derangements of normal physical function due to participation in sports, resulting from the rapid or repetitive transfer of kinetic energy”.
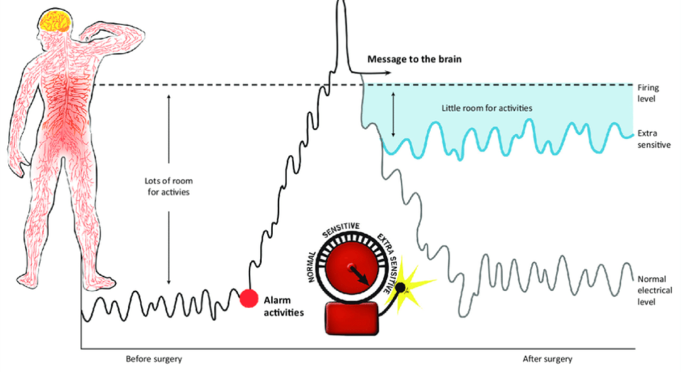
Injuries result in a measurable decrease in sporting performance Following injury, one may experience pain for a period of time, I’d like to think of pain as an alarm system (see Fig.3), it is how our brain detects and warns us of potential threats. In rare instances, these warning signals from our brain can turn unreliable due to a multitude of factors, resulting in a ‘false alarm’ and thus, pain occurs without evidence of actual tissue damage.
Pain is complicated
Fig.3 below shows that sometimes our brain can create an environment where our nervous system becomes hyperactive (particularly if you have sustained an injury to that area before), to the point where previously non-painful stimuli can become painful. This is known in medical terms as hyperalgesia, or an increased sensitivity to pain. The complexity of pain is well described in the literature. For example, in one study, researchers used an MRI to screen 3,310 individuals aged between 20-80, results showed that all individuals had signs of disc degeneration and disc herniations, but they experienced no pain20.
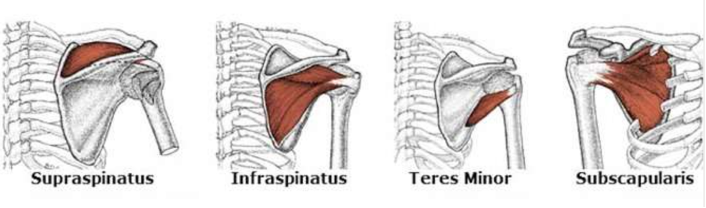
Similarly, a second study21 examined the shoulders of over 6112 people aged between 20-80 and showed an increasing trend of rotator cuff (see Fig. 4) abnormalities with age regardless of symptoms or shoulder dislocation. To quote the authors, “The prevalence of rotator cuff abnormalities in asymptomatic people is high enough for the degeneration of the rotator cuff to be considered a common aspect of normal human aging and to make it difficult to determine when an abnormality is new (e.g., after a dislocation) or is the cause of symptoms”.
So what is the takeaway? It means that many people out there are living their lives without pain and disruptions to their daily activities or performance, but an MRI would probably detect a disc bulge or a rotator cuff tear. Therefore, pain can be very misleading as there is not necessarily a clear-cut relationship between perceived injury/damage and the sensation of pain itself, which makes precisely identifying the true cause of any specific injury, a difficult task22 (unless, you feel intense pain and completely tear a muscle during a lift *yikes*, then It’s clear that lifting that weight was the inciting event, but it's likely there was a hidden, underlying factor that led to that injury, which is what I’m referring to here as a ‘difficult task’).
Exercise Technique and Injury Risk
As mentioned at the start of this article, you may have heard that there’s a specific way to do an exercise, or some exercises (such as deadlifts) are inherently bad and will lead to injury. That can’t be further from the truth, as there is not a lot of research backing up those claims, partly because there hasn’t been a well-designed experimental study that included both males and females while controlling for other physical, psychological, environmental, and demographical variables.
Hence, examining exercise technique's influence on injury risk would prove challenging as everyone differs anatomically (i.e., someone’s thigh bone length might be longer, or his biceps may insert 2-3cm further down on the arm than the other person).
This variation alters the amount of force going through each joint, determines how much force our muscles can produce23, and how an individual will move on a particular exercise. This is further complicated in that humans are not perfectly symmetrical, we may have one shoulder that’s higher than the other, or one arm muscle that’s stronger than the other side, and that’s normal!

A lot of personal trainers out there make a fuss about how everyone should move a certain way during a specific exercise, sometimes even stopping people mid-set to “correct” their posture, which can be really frustrating for people who are just getting started (and they end up not enjoying the exercise, or worse, quit going to the gym.
In fact, kinematic studies have shown that no matter how much you try to keep a neutral spine (defined as an individual’s relaxed standing posture where the stress on the spinal column and muscular effort required to maintain this alignment is minimal) during a deadlift, the lumbar spine (lower back) still flexes up to 50-80% of maximum flexion24–26.
Now, of course, there’s an important caveat here - which is that “good” technique matters, but there’s a lot more flexibility to that term than currently practiced by many. If the movement feels comfortable and you feel strong, and confident in that position, continue doing it, internal feedback (how you’re feeling) matters more than external feedback (observation), in this case.
Therefore, although the direct causes of injury are not fully understood, the available data suggest that poor intensity management may be a contributing factor. For instance, lifting a weight that exceeds the capacity of your tissues, with underlying factors such as high training fatigue, overall stress, and high training load 27,28, may increase the risk of injury. Nevertheless, it’s important to note that our bodies are highly adaptable and can adjust to the demands placed on them if they are scaled intelligently.
(Need personalized guidance on setting your lifestyle and training up for success? Apply for coaching here)
While there is a case to be made for poor form being a potential cause of injury, it is difficult to design a study that can directly investigate this factor as previously discussed. Inefficient movement can lead to poor load management, as differences in body position load the body differently, resulting in irregular or sudden spikes in tissue loading, and possibly leading to injury.
However, there is no single position that inherently determines the likelihood of injury. Instead, it is possible that injuries may be more commonly caused by poorly planned increases in intensity. In the few sections, I’ll discuss a few tactics to strategically lower your odds of injury.
Managing “Risk”
“There is some risk involved in action, there always is. But there is far more risk in failure to act”
Harry S. Truman
It’s unlikely we can definitively prevent injuries, as there are too many factors involved, sometimes life’s events can overwhelm us, or we don’t get enough sleep, and accidents simply just happen. Humans are complex, dynamic, and ever-changing systems with cells and organs that interact with one another, adapt, and evolve29 – No human being is the same as another, which holds true, even for identical twins. Given this complexity, what matters is to best understand injuries and how to get back from one.
Instead of injury prevention, a more evidence-based approach would be risk reduction. Think about it, during our day-to-day lives, every decision we make has a consequence and thus, we unconsciously perform a cost-benefit analysis, where we weigh the benefits and drawbacks of each decision. For example, when we ask our superiors at work for a promotion or pay increment, we risk being turned down. When we choose to drive to reach our destination earlier instead of walking to our destination, we risk the odds of getting into a road accident. Does the presence of risk mean we should avoid something altogether? I don’t think so, I don’t think anyone in their right mind would want to walk to work every morning instead of taking a taxi or the bus (unless you live within walkable distance), you get the idea.
If fatigue, stress, and poor load management, as described above are the key drivers of how and why injuries happen, then managing these factors would be the next logical risk-reduction strategy. As alluded to earlier, these factors are largely psychosocial in nature, again showing how our minds are deeply interconnected with our body30–32. Let’s go deeper into these factors, starting with load management. A popular injury prevention framework termed the acute:chronic workload ratio (ACWR) was developed by TJ Gabbett33 and a few other researchers in the past couple of years. Since then, it has been widely used by sports coaches and physiotherapists (particularly in football and rugby) in the past decade to monitor and track an athlete’s average training load. However, this system of monitoring workload has been critiqued recently in the literature, with some authors citing that the system may be flawed conceptually and methodologically, and whether ACWR predicts injury incidence (or occurrence) independently of other risk factors is unclear, highlighting the need for further research in this area34,35.
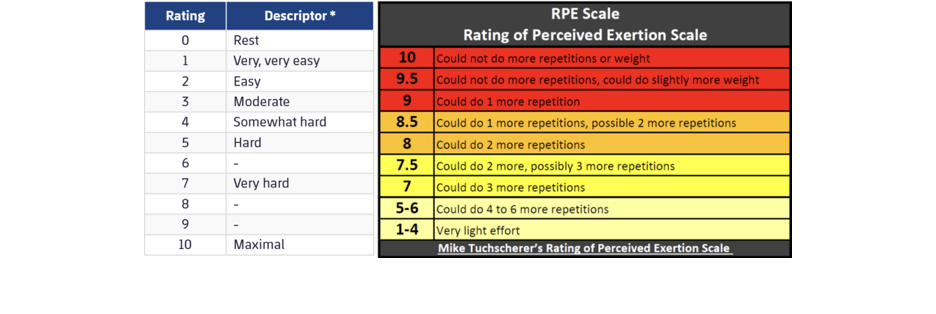
Fatigue, on the other hand, can be objectively measured by external intensity, through the load (or weight on the bar) used, and internal intensity, through the rating of perceived exertion (RPE) scale (see Fig.5). The scale can be measured either through session RPE after the workout or after each exercise. RPE is great as an autoregulation tool to manage fatigue because it is free to use with no equipment needed, accounts for variability in performance (you have good days and bad days). This makes training sustainable over the long term and gives the lifter autonomy and self-efficacy over a typical workout session.
Now for progression to occur, appropriate exercise selection must be coupled with graded, stepwise increments in intensity or volume. if the athlete or individual is exposed to too much (load), too soon, he/she may get close to the injury zone. Similarly, too much training volume using an unsuitable exercise can lead to high fatigue during the session itself and even on the days after the session. A higher fatigue exercise session would necessitate a longer recovery period due to a bigger recovery “hole” from improper program design (i.e., a deadlift in general is more taxing on the central nervous system than say, a bicep curl). Therefore, it’s imperative that all aspects of program design from exercise selection to total workload be tailored intelligently to suit your goals.
Need personalized guidance on setting your lifestyle and training up for success? Apply for coaching here
Keep the training load consistent.
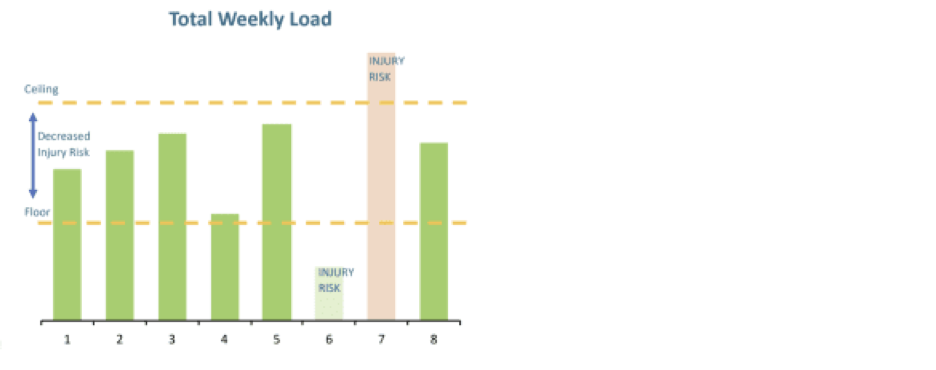
Let’s say your travel frequently for work, or other life commitments just get in the way of your health/fitness routine. These events may last for weeks to months, and when you’re eventually returning to your workout routine, you may feel great and recharged. However, your fitness levels have likely decayed36, and your body might not be ready for high training volumes (workload), as it previously was. As you’ve read in the previous section, sudden spikes in training load (volume or intensity) increases the likelihood of injury (see Fig.6). Therefore, we must be cognizant of the amount of weekly training load that we’re performing. A great tip is to take some time to scale back the training load to a slightly lower level than where you were before the hiatus, and then gradually increase it. There’s a phrase I’d really like that summarizes this entire paragraph well, “There’s no inherently bad exercise, only the one you’re not prepared for”.
Practice Mindfulness and Stay Calm
As mentioned previously, injuries are partly contributed by psycho-social factors, which means that stress, especially chronic stress37, and emotions such as anxiety all affect our physiology and therefore our training performance38. Being in a state of chronic stress causes an overproduction of pro-inflammatory cytokines (messengers that stimulate inflammation throughout the body). Inflammation that persists for too long is linked to a host of age-related diseases, such as cardiovascular disease and diabetes, and musculoskeletal problems such as knee osteoarthritis39. The study that I cited earlier by 30 concluded that psychosocial variables and psychological interventions can influence injury risk in athletes. Knowing this, it’s important that we prioritize our mental health as much as our physical health if we want to prevent injuries from happening.
Sweep the Ego aside & Track your workouts
If you’ve made it this far, great! I hope you’ve learned a great deal about reducing your risk of injuries in the weight room. We’re on to the last section, and this is somewhat trivial and a no-brainer but I thought I’d highlight these two as it still plays a role in injury prevention.
Let’s face it, besides the plethora of health benefits resistance training provides40, we all want to improve the way our body looks and feel confident in it. That being said, Strength and muscle gains take a longer period of time to accumulate due to lower androgen levels (androgens are a group of hormones that give males their specific characteristics, females also have them, but to a lesser extent) due to aging. We simply don’t recover from “hard” workouts as quickly as when we were in our 20’s. As a result, progress may come slowly, especially after one crosses the beginner phase, where most of the gains in strength training are largely due to neural adaptations. This is where your brain gets better at recruiting more motor units (or muscles). Additionally, as you get exposed to the same exercise again and again, your body becomes accustomed to the exercise, and thus, gets more efficient at performing the movement, a scientific term called “motor learning”.
So what is the takeaway from all of that? Two key points. First, be patient, and committed to a workout routine that you find sustainable for your lifestyle, be it two, three, or five days a week (I’d recommend a minimum of two days a week). If you’re lifting for the next two to three decades (given the health benefits, I hope you do), the occasional vacation or hiatus wouldn’t matter. Second, Find a way to track your training load (be it a paper journal, mobile app, or spreadsheet), and increase it over time. That’s it! I hope this article has shed some light on resistance training, the risks of injury (which are really low), and how to set yourself up so you don’t fall prone to injuries. Some of the topics above, such as pain and injury type were discussed briefly and will be further explored in later articles.
References that were cited in this article can be viewed here

Marcus Oon
Marcus is a practicing physiotherapist and strength & conditioning specialist located in Singapore. He completed his honor’s degree at the Singapore Institute Of Technology - Trinity College Dublin, and his Strength & Conditioning certification at the National Strength & Conditioning Association.
Found this article informative?