
 thrust joint manipulation, it sure feels great!")
Table of Contents
- Introduction
- What is joint manipulation
- Going forward with the term 'Manual Therapy'
- Effects of 'Manual Therapy'
Introduction
I was inspired to write this article after a recent interaction with a client, who shared about going for multiple chiropractic sessions in the past, which only provided temporary relief for her back pain. We had a short discussion about the effects of such treatments on the body and brain. To her surprise, and to quote her exact words "really something new to me, lol".
If you've suffered or are suffering from any kind of pain, especially back and neck pain, you might have had close friends and family who suggested you visit a chiropractor to 'fix' your spine. After all, most people don't fully understand the extent of a chiropractor's or physiotherapist's (*coughs* massage) practice unlike traditional medicine (at your family clinic), but that's a topic for another day. Now I would like to point out here that chiropractors are not medical doctors, and do not have a regulatory body governing their practice in Singapore. It is also considered an 'alternative treatment' to conventional medicine, although 'alternative' may not justify its increasing popularity and success, as statistics reveal.
Approximately 1 in 3 people suffering from lower back pain in the United States seek the help of a chiropractor, this trend has risen over the past decades, with spending on chiropractic care rising from between US$2.4 and $4 billion in 1988 to $5.9 billion in 2006, with a recent report forecasting a market size of up to $16.9 billion in 2027. A post made by Harvard Professor Steven Salzberg stated how US Medicare wasted an alarming $497 million in funding for chiropractic treatments. The reason for sharing this data is twofold. First and foremost, it is clear that people are spending more money than ever to resolve their pain, and therefore, healthcare practitioners should be providing evidence-informed, value-driven care. This way, we can reduce unnecessary spending on musculoskeletal conditions such as lower back pain, which is the number one global cause of disability, posing a huge socioeconomic burden. (some clinics are insurance-claimable, needless to say, excessive claims will result in healthcare inflation, some way or another), although good progress has been made in recent years.
This article will first discuss what spinal manipulation or joint manipulations (they will mean the same thing in this article) are all about, address some myths, and finally, discuss some of their mechanisms and effects on the brain and body so you can make an informed decision on whether its really necessary for you to get 'cracked'. Besides, it can also be a topic up for discussion with the chiropractor if you do decide to visit one.
Disclaimer: While there are certainly evidence-informed chiropractors who provide effective treatment, as with any profession, there are some practitioners who may engage in unethical practices solely for the sake of gaining attention or promoting misinformation about the true effects of certain treatment techniques. It's important to keep this in mind as we delve into today's topic.
What is joint manipulation?
When you're in chronic pain (often defined as pain lasting more than 3 months), nothing beats coming into a supportive environment, where the clinician understands (or at least tries to) and validates your pain experience. Even better when you're told that the cause of your pain is simply a bone that needs to be shifted back because it's out of alignment. Ok, maybe just the former is true, but I didn't pull this statement out of nothing. One of the likely reasons for this is that the longer pain persists, the further it deviates from the biological model (i.e., potential tissue damage), and the more it is associated with other drivers of pain, such as psychological, social, and environmental factors1,2.
Furthermore, studies suggest that although chiropractic (mainly the cracking part) has no clear scientific basis, the visit to the chiropractor itself — with the patient's expectation of change, a simple mechanical explanation for diagnosis, and feelings of empowerment all result in enhanced recovery, particularly for chronic pain sufferers. This is often referred to in research journals as therapeutic alliance3,4, whereby both clinician's and patient's goals align, which has been shown to improve disability and functional outcome measures5.
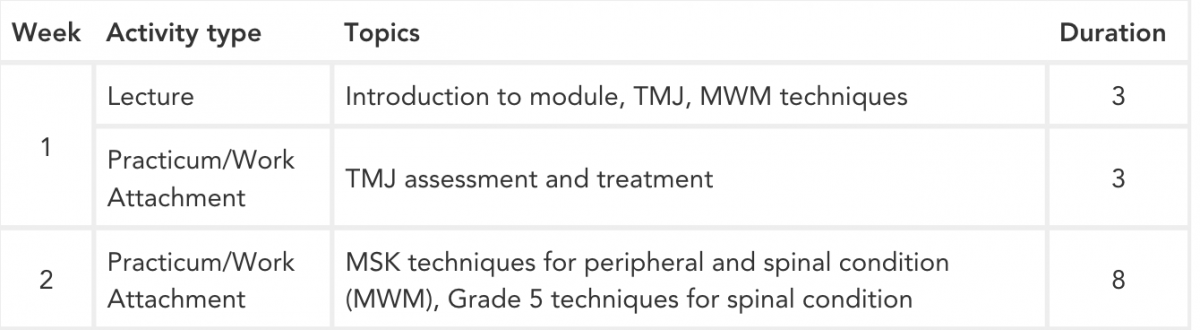
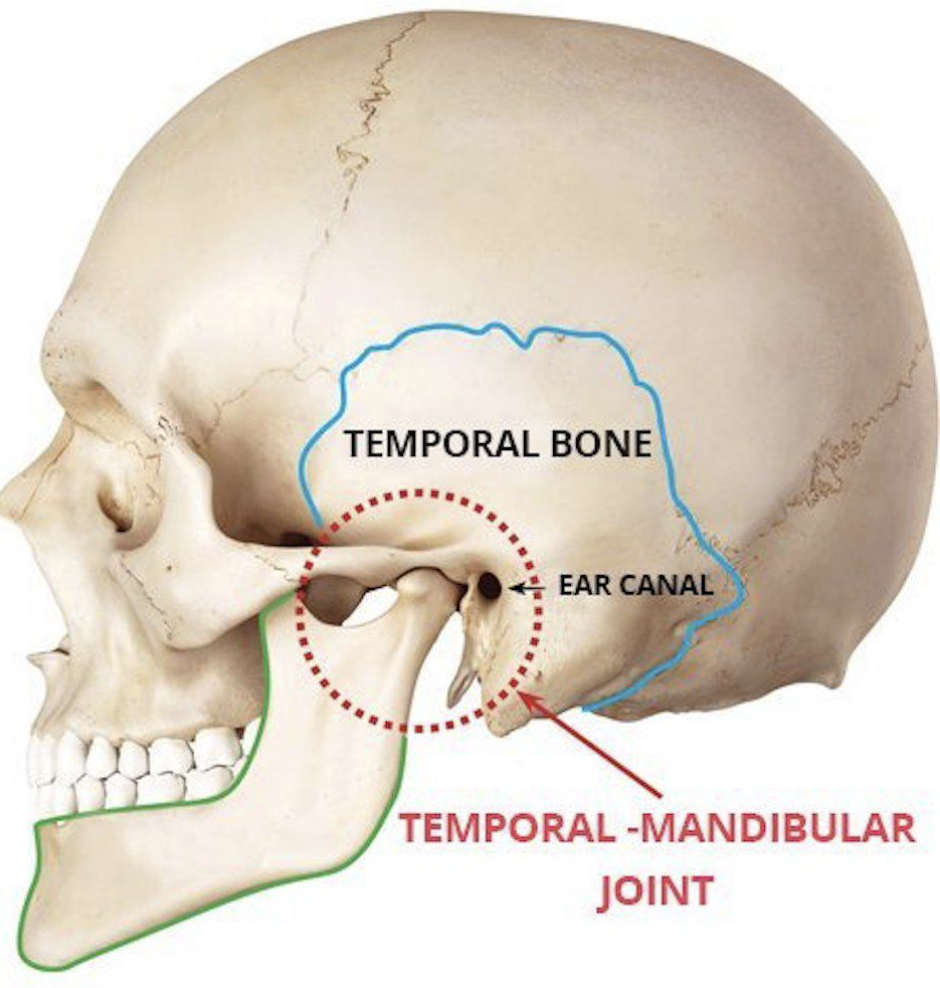
Most people believe that joint manipulation is a skill exclusive only to chiropractors, except it is not. (I'm going off-tangent here for a bit, bear with me) In fact, during my undergraduate years as a physiotherapy student, we had to pick one out of several elective modules during our final year. As you may have predicted, one of them (Fig.1) involved the learning of advanced manual skills such as temporomandibular (TMJ) joint assessment, treatment (the joint that connects your jaw to your skull, in Fig.2), and Grade 5 techniques, which are basically joint manipulations, or the 'science' of popping joints with the aim of reducing pain and increasing movement available at that joint.
With that out of the way, let's circle back to the main point, what are joint manipulations? Essentially, it is a hands-on technique, where a high-velocity thrust is applied to the joint that is assessed to be "stiff" or hypo-mobile. The cervical spine (neck) and lumbar spine ( lower back) are the most frequent areas where manipulation is applied.
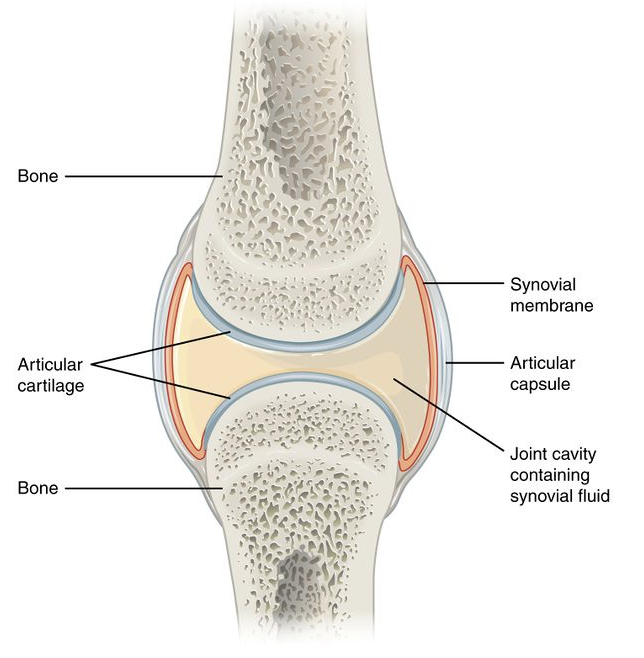
The "pop" sound occurs when a distraction force (produced by the practitioner) is applied to a joint, resulting in cavitation within the joint's synovial fluid. To quote an excellent study on this topic;
"Cavitation is the formation and activity of bubbles in fluid through the local reduction of pressure within the fluid. During joint cracking, this pressure reduction is caused by the separation of the joint surfaces. The bubble grows very rapidly to a maximum size, before immediately and violently collapsing as the synovial fluid rushes into this lower-pressure region"
Unsworth et al. (1971) in “Cracking joints”. A bioengineering study of cavitation in the metacarpophalangeal joint
After a manipulation, some people may experience immediate pain relief and relaxation. In rare cases, there may be slight discomfort and soreness that typically dissipates after a few minutes. Now there are some claims online (particularly those with a vested interest), that spinal manipulations:
1. 'Corrects' spinal misalignment,
2. Improves range of motion
3. Releases pressure on the nerves, and many more.
4. Helps with many conditions such as, but not limited to
- Headaches
- Lower back pain
- Neck pain
- Sciatica (better addressed as radicular pain)
- Disc herniations
- Scoliosis
- Dysmenorrhoea (or menstrual cramps)
But are joint manipulations really that amazing? i'll address each of these in my next article, so stay tuned for that!
Before we get into the specific effects of manipulation, I'd like to first define and expand on what manipulation is and where it currently stands in physiotherapy practice, so that you get the entire picture. If you're not interested or don't have the time, feel free to skip the next section and read here instead.
? Like what you're reading so far and find it insightful?
Stay in the loop and never miss a new post by subscribing to my newsletter here.
Going forward with 'Manual Therapy'
As described earlier in this article, joint manipulations and mobilizations is a skill not exclusive to chiropractors, although admittedly, they are most recognized for employing this particular intervention. For example, In 1988, the American Physical Therapy Association (APTA) defined mobilization/manipulation as “a manual therapy technique
comprised of a continuum of skilled passive movements that are
applied at varying speeds and amplitudes, including a small amplitude/high-velocity therapeutic movement", where Manual Therapy, a broad umbrella term, is defined as "the use of hands in a curative and healing manner or a hands-on technique with therapeutic intent".
The important word here is 'passive', meaning the patient is not actively engaged in the treatment, and yes massage is considered a passive treatment, as well as dry needling (see Fig.3). Numerous studies have demonstrated that active treatment approaches, such as exercise therapy, typically yield superior long-term outcomes in terms of self-reported pain and functional disability levels compared to passive treatments alone. Nevertheless, passive treatments still hold value in cases where the adoption of exercise therapy is hindered by pain-related avoidant behaviors (meaning people don't do their prescribed exercises because of pain). These passive interventions have been shown to provide immediate analgesic effects, meaning they can promptly alleviate pain, which potentially facilitates subsequent engagement in exercise and other active therapies.

In recent years, the terms "thrust" and "non-thrust" have since been established, to better distinguish the two terms, manipulation and mobilization respectively (watch the video below to learn more about the differences between both). These techniques originated from Geoffrey Maitland, one of the pioneers in the field of physical therapy. In the early 1960s, Maitland established a system for assessing and managing musculoskeletal conditions through manual therapy, which is now widely utilized by modern physiotherapists, manual therapists, osteopaths, and even some chiropractors. (Again, the emphasis on manual therapy within physiotherapy programs depends on the institution where they received their training. Some physiotherapy programs place significant emphasis on manual therapy techniques, while others may not prioritize it as heavily).
It's also important to note here that these techniques are applied in a continuum, where modifications to velocity and amplitude are dependent on the continual reassessment and evaluation by the physiotherapist, to achieve the desired clinical outcome (a reduction in pain resolution or an improved ability to raise your hand overhead, for example).
These techniques are primarily utilized to alleviate pain or enhance the range of motion in specific joints. The underlying mechanism behind these techniques will be explored in detail in the following section. However, as mentioned in my previous article, pain is complex, and pain by itself is not solely indicative of structural or tissue damage, which manual therapy aims to address.
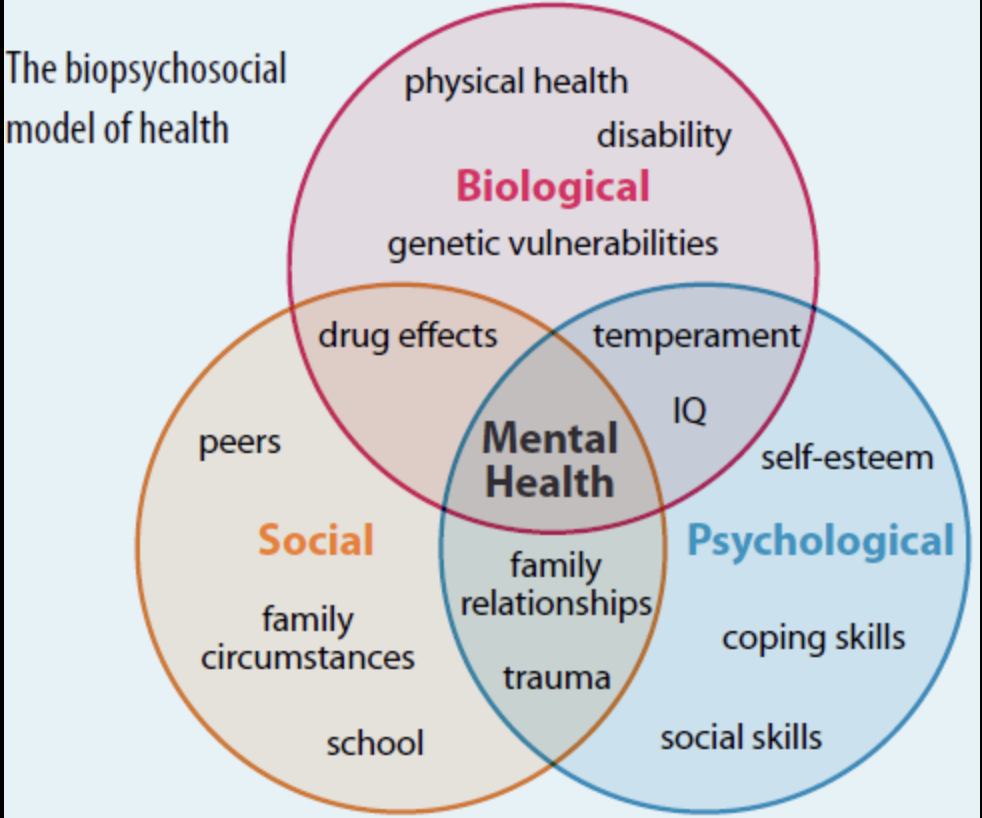
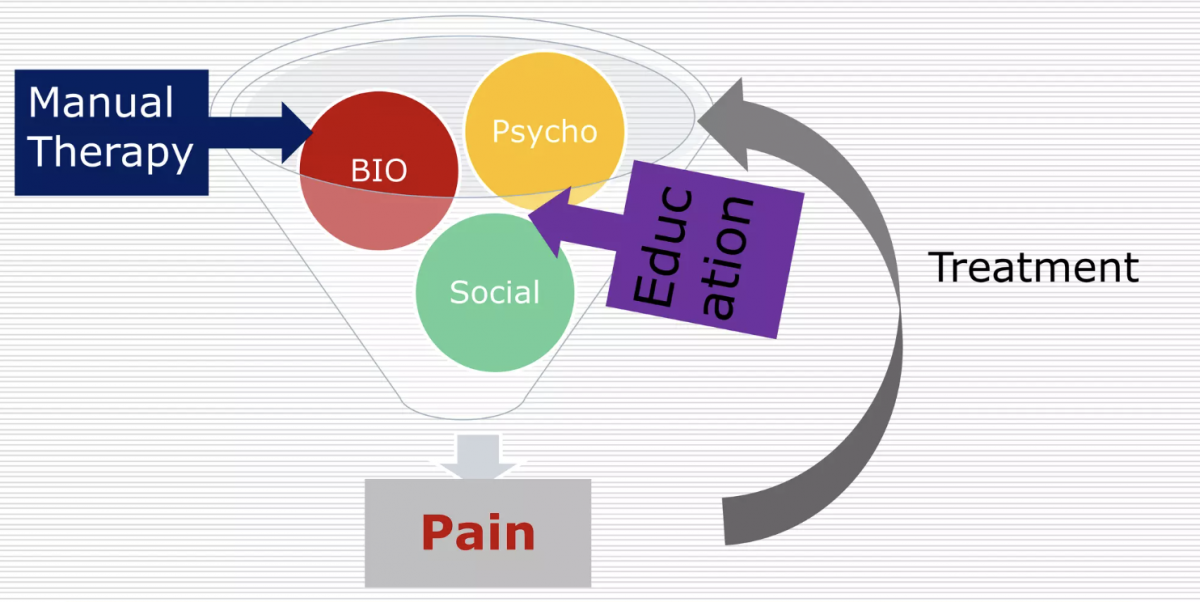
This understanding is now widely recognized by healthcare professionals, thanks to the influential work of Professor Lorimer Moseley and a group of pain researchers. They succinctly explained this concept in a YouTube video, which has garnered over 400,000 views. The biopsychosocial model of pain, initially proposed by George Engel in 1977, sparked a significant shift in pain research. This model emphasizes that a person's medical condition should not be exclusively attributed to biological factors but also considers the psychological and social aspects (refer to Fig 4 & 5). It is crucial to consider this multifaceted nature, especially with persistent pain disorders, as psychosocial variables such as depression, anxiety, and distress have been shown to be strong predictors12-15 for the development of chronic pain.
Effects of 'Manual Therapy'
How it compares against other therapies
Despite the extravagant claims made by certain chiropractors in Singapore, as discussed here, spinal joint manipulation alone is not extraordinary. Multiple research studies6-11 exploring spinal manipulation against sham treatment or placebo (a placebo is any treatment with no active properties, i.e., receiving a sugar pill while being told it's a drug of interest) showed similar effects with regard to pain and disability. However, many studies investigating spinal manipulations against sham/placebo were poorly designed, which makes drawing firm conclusions challenging.
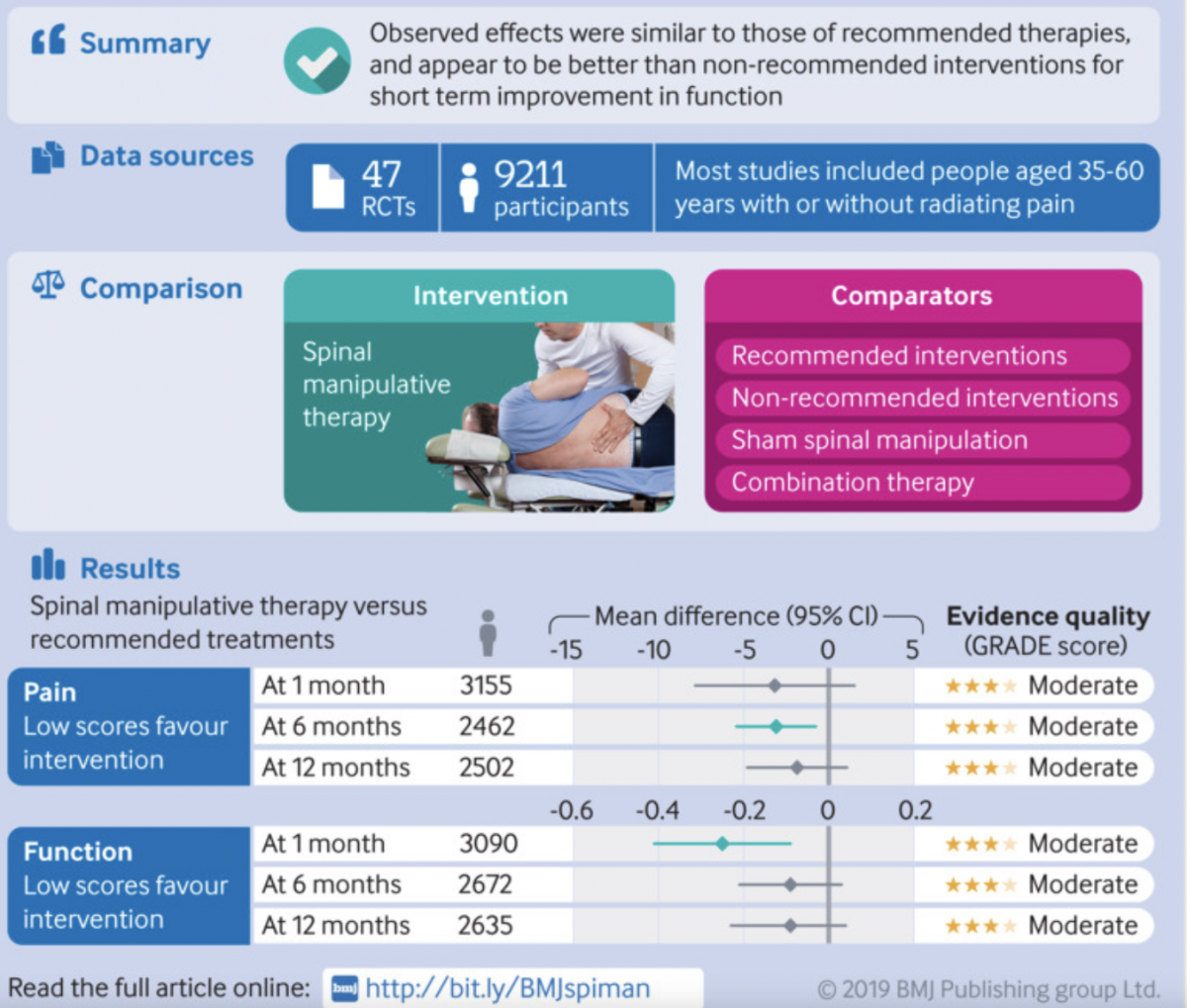
However, when we examine research comparing spinal manipulation to other treatments, a meta-analysis reveals that there are no clear superior benefits of spinal manipulation over conventional care options such as painkillers and back pain education. This corroborates with another meta-analysis conducted by Rubinstein et al. (2019), which indicated that patients with chronic back pain only experienced short-term improvements in function that diminished after 6 months.
Similar to the previous study, the authors then concluded that spinal manipulation was not more effective than other recommended interventions like exercise therapy, and back pain education. (see Fig. 6) Based on the figure below, we can see that differences in function between groups one-month post-treatment showed a small statistically significant difference.
For pain, although there was a significant difference at 6 months, the effect size was, according to the authors, small and not clinically relevant (meaning the findings have limited practical applications in the real world).
So, what does all of this information mean?
It suggests that perhaps there are more effective ways to utilize your time (and financial resources) during your visit to the physiotherapist/chiropractor. If the clinic you're currently attending only involves lying on a bed for 30-45 minutes while receiving 'back cracking', massages, foam rolling, ultrasound, or dry-needling, it might be worth considering alternative options.
It's important to seek comprehensive and evidence-based treatments to address your specific needs. However, if receiving ONLY passive treatments falls within those needs then it's not all that bad, as long as the physiotherapist or chiropractor duly informs you of the treatment effects, potential risks, and alternative therapy options that have been proven to be more effective and provide long-term benefits (such as exercise coupled with education about back pain).
(if you know the treatment is only going to provide short-term relief, and you'll have to come back every 1 or 2 weeks for the same treatment, you'll probably ask for something else... right?)
Biological Mechanisms of Manual Therapy
If something sounds too good to be true, it probably is
- A Very Wise Man
How and why does spinal manipulation/mobilization create an immediate pain-relief effect?
There are many hypotheses available on how manual therapy such as massage and manipulation works to effect these changes, but I'll briefly discuss a few.
Ever hit your knee or foot on a hard object and found yourself instinctively rubbing the painful spot?? This simple, automatic behavior that often happens immediately after a painful experience is rooted in a scientific and biological concept.
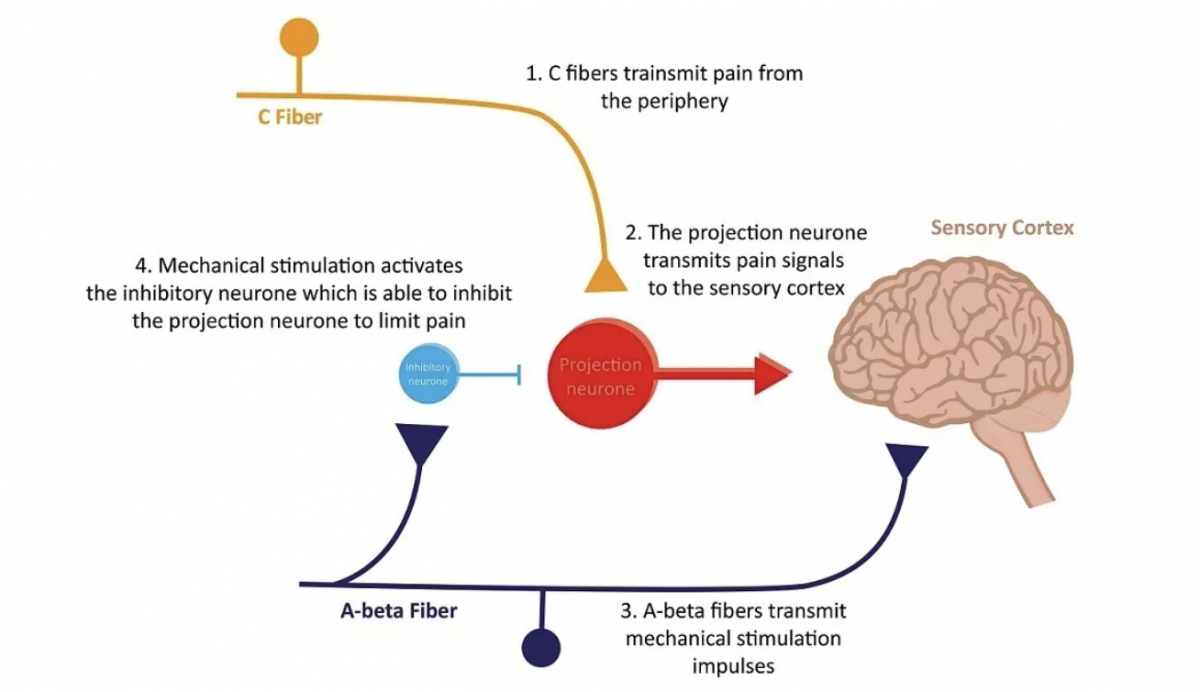
First, the Pain Gate theory, introduced by Ronald Melzack in 1965, suggests that the electrical signals that potentially signal pain from the peripheral nervous system (or the nerves that branch out from the brain and spinal cord) are subject to a number of modulations in the spinal cord by a “gatelike” mechanism before the experience of pain is transmitted to the central nervous system (your brain or spinal cord, see Fig.7) Rubbing the painful spot or getting a massage in this case, is the mechanical stimulation that "closes" the gate and reduces some of the pain you experience at that point. Note here that this is purely a central nervous system response that alters pain processing, and NOT the release of "trigger points", or "knots" which have yet been proven to exist despite decades of scientific debate.
However, just like how pain can be modulated through upstream methods like this, there are also downstream methods by which the brain modulates the amount of pain you feel, and these are contributed by social, and psychological factors as explained earlier. Anxious thoughts, negative emotions, memories, poor past experiences with pain, and negative social feedback can amplify or "open" the gate, thereby increasing the amount of pain you experience.
The second theory proposes that thrust manipulation diminishes the summation of electrical impulses originating from the nerves in the lower back musculature, resulting in a dampened sensation of pain at the level of the spinal cord. To put it simply, this decrease in electrical impulses leads to a reduction in the perception of pain in the brain.
A systematic review of 10 studies also found a small but non-significant positive effect of thrust manipulation on local pain threshold — which means that pain tolerance in that region increased — and a favorable, significant increase in remote pain threshold. This means that thrust manipulation indeed has effects that extend beyond the local area (back or neck) of application. All of these findings are congruent with the other two hypotheses previously mentioned, that spinal manipulation alters pain processing and sensitivity at the level of the brain and spinal cord.
Nevertheless, the authors concluded that most of these effects only resulted in an immediate improvement in pain, and whether these improvements in pain sensitivity lead to a clinically significant or meaningful improvement in function is still unclear.
Potential harms
While the benefits of spinal manipulation are notable, it is crucial to acknowledge that harms and serious adverse events are relatively rare. However, there have been isolated case reports of cauda equina syndrome, fractures, and neurological or vascular compromise occurring in both the cervical (neck) and lumbar (lower back) regions as a result of spinal manipulation16-19. Serious adverse events that have happened are also rarely reported in medical literature.
Therefore, if you still decide to go ahead with an "adjustment" despite reading the above, it may be prudent to seek medical clearance from a board-certified physician to assess your suitability for spinal manipulation, as certain factors are known to increase the risk of adverse events20.
REFERENCES
Numbered citations in this article can be found here
Hope you learned something from this piece! You can help me by:
1) Sharing this article with friends and family, if you think it'll help them. Links to share this article on social media channels can be found below
2) Leave comments for any topic suggestions or if you have any questions (I answer every one of them!)

Marcus Oon
Marcus is a practicing physiotherapist and strength & conditioning specialist located in Singapore. He completed his honor’s degree at the Singapore Institute Of Technology - Trinity College Dublin, and his Strength & Conditioning certification at the National Strength & Conditioning Association.
Found this article informative?