

This is a continuation of the previous article: The Science Behind Back "Cracking": What Happens to Your Body Afterwards?, If you haven't read that yet, I highly suggest reading it before this one.
This article aims to address certain claims made by certain chiropractors. If you can't recall what those claims are, don't worry. This article is structured in sections, with each paragraph dedicated to a specific topic/condition, providing valuable insights and information.
Here, I will attempt to briefly review what is known about manipulative treatments for each of these conditions with supporting literature.
Without further ado, let's get crackin' dive into today's piece.
Claim #1: Spinal Manipulation corrects spinal misalignment and Posture (or even Scoliosis!)
THREE reasons why this is false.
First, this claim assumes that the pain you're experiencing is solely attributed to a biomechanical cause, meaning your posture and spine deviations are CAUSING your pain. In my previous articles, I extensively discussed the topic of pain, which you can access here. In short, know that pain is not solely influenced by biological factors (like an injury), there are other factors that play a significant role in shaping our pain experiences, such as our environment, and psychological state.
In a landmark study conducted by Lederman (2011), it was unequivocally established that there's a lack of association between your posture, shape, or structure of your spine and pain, particularly when it relates to back pain.
Furthermore, a comprehensive study of 692 individuals reached a similar conclusion, highlighting the inadequacy of these factors as reliable predictors for the onset of future low back pain.
To quote a sentence from my first article: asymmetries and imperfections are part of being human, and it is perfectly normal!

Needless to say, this excludes severe injuries and spinal deformities such as spinal fractures and scoliosis.
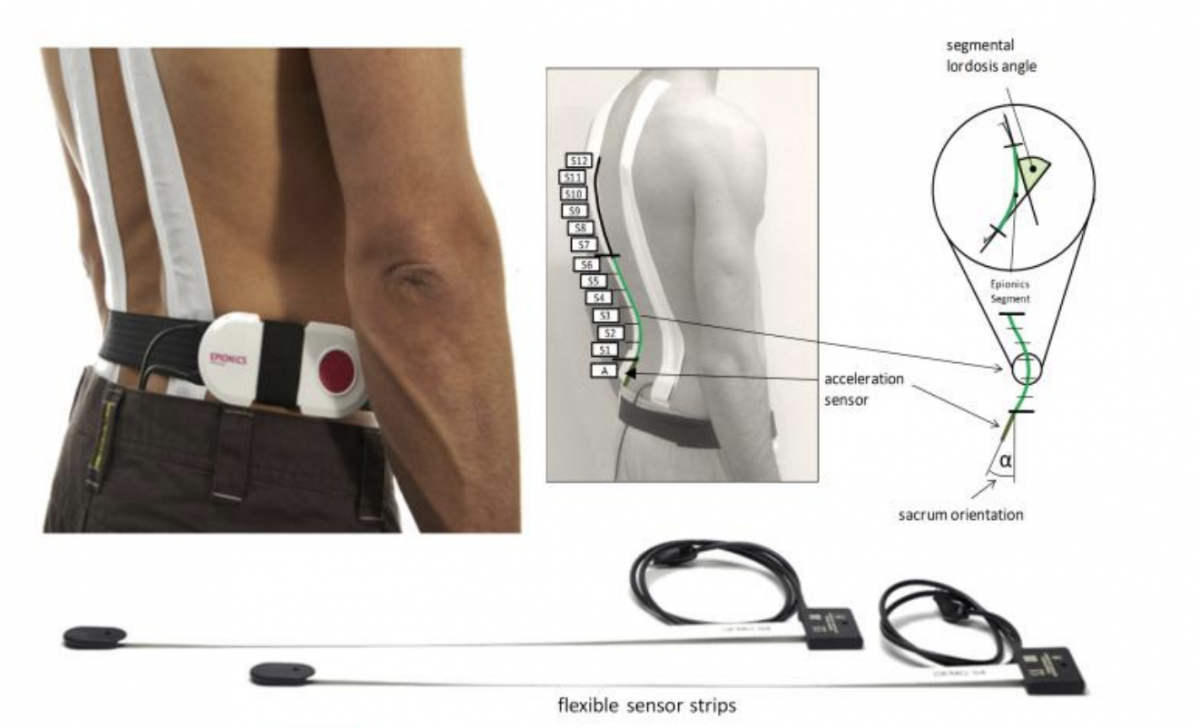
Next, this study examined the standing posture of 353 subjects (athletes and non-athletes) without low back pain and 83 others with chronic low back pain using a flexible spine movement detection device (see Fig.1). Given the device's adaptability, it is well designed to assess lumbar spine shape and rotation of the sacrum. What the authors found was that standing posture and orientation of the lower spine were highly variable and individual regardless of age, gender, BMI, height, or bodyweight! (meaning no differences in posture were found between those who had lower back pain and those without).
Lastly, it's not easy to change the shape of your spine, as evidenced by this study, which took several teenagers with scoliosis and assigned them to two groups: one with a corrective brace and one without.
The researchers then followed them for 5 years! At the end of the study, there were differences in spinal curve progression between the groups. However, when the researchers conducted a follow-up months after the initial review, they found that the differences in spinal curvature were similar in both groups. This indicates that wearing a "corrective" brace for 5 years did not have a clinically significant effect on the normal progression of scoliosis or bring about a change in the spine, let alone a joint manipulation, which only requires a minimum of 202 newtons (N) or 20 kilograms of force to perform.
If it was that easy to change our spines, we'd grow taller just by "hanging" on pull-up bars, where our spines will be taking the majority of our body weight in addition to gravity, and we'd have multiple spinal fractures just from sprinting, given the large vertical ground reaction forces (GRF) of up to 2000 Newtons (N), acting on our spines.
But we all know that's not true.
It'd be terrible for us as a species if our spines were that fragile.
Claim #2: Spinal Manipulation improves range of motion or range of motion at a specific segment of the spine
A systematic review of fifteen independent studies showed that spinal manipulation produced a positive, albeit modest effect on cervical (neck) range of motion. However, the authors also noted that such improvements in range of motion were not seen in the jaw, the lower back, and the pelvis after spinal manipulation.
However, it is important to note that the authors of the study recognized a limitation in their review, as they did not assess the impact of spinal manipulation on pain levels and long-term outcomes, focusing solely on its immediate effects on range of motion (ROM). Their reason for doing so was due to the lack of available evidence in the literature.
Additionally, the natural course of various musculoskeletal conditions, including shoulder pain, neck pain, and lower back pain, often exhibits favorable outcomes over time, making it unclear if the modest improvement in range of motion can truly translate to meaningful real-life scenarios where the factor of time becomes a confounding variable.
Finally, a systematic review of 10 studies by Nim et al. (2021) showed that a "specific" spinal manipulation (meaning a clinician-determined site, where they palpate and supposedly locate the "affected" vertebra") has no difference in pain and disability outcomes over one that is delivered more haphazardly at an entirely different region of the spine. This is further supported by another randomized trial which concluded that the application site of spinal manipulation is not important for clinical outcomes such as stiffness or pain.
From a musculoskeletal clinician's perspective, this finding brings about a seismic paradigm shift in assessing and treating spinal pain — What purpose do spinal manipulation and mobilization treatments serve if we cannot accurately and reliably pinpoint the specific spinal segment using manual assessment techniques?

? Like what you're reading so far and find it insightful?
Stay in the loop and never miss a new post by subscribing to my newsletter here.
Claim #3: Spinal Manipulation Helps with Headaches

There are various types of headaches, each with different diagnostic codes, categorized into primary and secondary headaches. However, the two most common ones by far are:
1) Migraines, ranked the third–highest cause of disability worldwide in both males and females under the age of 50 years.
2) Tension-type headaches, which can be further classified as infrequent, frequent episodic, or chronic, have a lifetime prevalence ranging from 30% to 78% in the general population. These are ordered with respect to the increasing level of disability it causes — meaning chronic types cause more disability than infrequent etc.
When we look at the literature, a systematic review by Astin and Ernst in 2002 stated that no definitive conclusions can be made with the data available at that time, despite claims that spinal manipulation can treat headache disability and pain.
The authors also noted that the clinical trials at that time had several methodological limitations and it is unclear if the positive effects on pain relief seen in many of these studies were due to other factors such as patient expectation and personal attention (placebo effects) provided by the clinician, I have discussed this phenomenon prior in my previous article and how it affects clinical outcomes.
However, a recent systematic review by Rist and colleagues in 2019 demonstrated some potential benefits of spinal manipulation in reducing the frequency and pain intensity of migraines. It is important to note, however, that these findings are preliminary and do not establish a causal or strong association (meaning we can't actually say it HELPS migraine pain directly).
Claim #4: Spinal Manipulation helps with lower back pain
This has been addressed in my previous article here.
Claim #5: Spinal Manipulation helps relieves symptoms of Sciatica (radicular pain)
A clinical prediction rule for identifying patients with low back pain who would likely benefit from spinal manipulation was developed by Childs and Colleagues in 2019. Clinical prediction rules help clinicians decide on the best course of action regarding the management of certain conditions.
After a rigorous trial, the researchers came up with five criteria and they found that patients who met at least 4 out of the 5 criteria had a 92% chance of a successful outcome from spinal manipulation at 4 weeks.
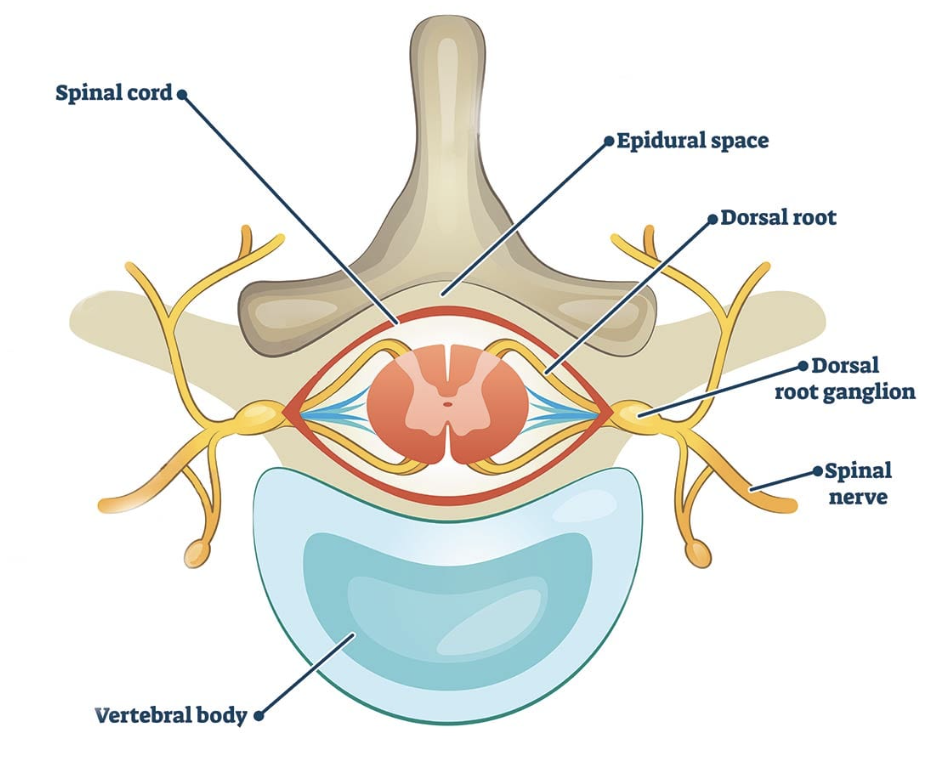
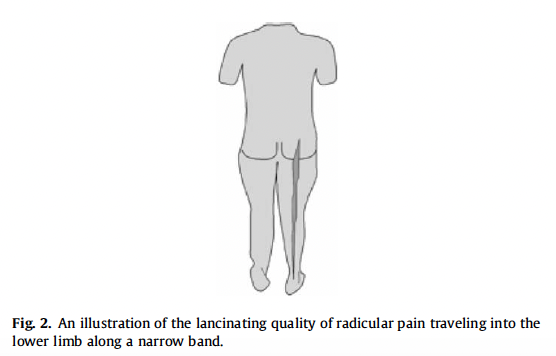
One of the 5 criteria states that the patient should have no symptoms distal to the knee, meaning there should be no pain going down the leg, which is typical of radicular pain, usually caused by a disc herniation or inflammation of the dorsal root ganglion (a bundle of sensory nerve fibers which lies between adjacent vertebrae, see Fig.1). This corroborates with the results of another study which states that "the risk to benefit ratio of spinal manipulation is unacceptably high for patients with radicular symptoms or signs associated with prolapsed discs and neck pain".
What all this means is that perhaps spinal manipulation isn't a good idea if you're having electrical-like pain going down the back of your leg, particularly if you've been having it for a while.
Claim #6: Spinal Manipulation helps with menstrual cramps

This idea that spinal manipulation helps with menstrual (or period) cramps has been suggested by certain practitioners.
This hypothesis suggests that manipulations increase spinal mobility, which in turn may improve blood supply to the pelvis and potentially alleviate pain.
However, a Cochrane systematic review (one of the highest-rated scientific journals) in 2006 of two trials showed no evidence that manipulation helps in relieving menstrual pain, and is no more effective than sham manipulation. An overview of dysmenorrhea (menstrual cramps) by the American Academy of Family Physicians also listed Spinal manipulation under ineffective treatments for such occurrences.
This is further supported by two systematic reviews in the last decade — showing that spinal manipulation had no significant reduction in pain and that more research is needed in order to ascertain its utilization in clinical practice — although, at this point, based on the data we have, it is extremely clear that the effectiveness of spinal manipulation in treating menstrual pain is dubious at best.
? Like what you're reading so far and find it insightful?
Stay in the loop and never miss a new post by subscribing to my newsletter here.
Bottom line
While spinal manipulation can be beneficial in certain situations, it is important to recognize that it is not essential and does not deliver the exaggerated effects that some practitioners may suggest. Instead, exercise therapy and education remain the fundamental pillars of musculoskeletal pain treatment and management.
With the conclusion of this article, we have covered the topic of spinal manipulations in depth. However, if you feel that there are any additional aspects or claims that have been overlooked, please leave a comment below or email me, and I will make sure to update the article accordingly.
In the upcoming articles, we will venture into the realm of strength and conditioning, delving into topics such as
- Waist circumference measurements, and what it tells you about your health.
- What subcutaneous/visceral fat is and how to lose them for good (or at least down to the level where you're not at risk for major diseases, even if you're not interested in having washboard abs).
Hope you learned something from this piece! You can help me by:
1) Sharing this article with friends and family, if you think it'll help them. Links to share this article on social media channels can be found below
2) Leave comments for any topic suggestions or if you have any questions (I answer every one of them!)

Marcus Oon
Marcus is a practicing physiotherapist and strength & conditioning specialist located in Singapore. He completed his honor’s degree (with Merit) at the Singapore Institute Of Technology - Trinity College Dublin, and his Strength & Conditioning certification at the National Strength & Conditioning Association. He is also an active member in the NSCA's Health and Wellness, Powerlifting, and Sports Medicine/Rehabilitation Special Interest Groups.
Found this article informative?